Discography - Operative techniques in spinal surgery
Dr. P.S.ramani has over 20 discs on operative techniques in spinal surgery. Selected and common 11 discs are selected here for display and playing on U-tube. Others can be made available on request.
The full set of 11 discs is available for sale and Dr. Ramani can be contacted for the same on drpsramani@gmail.com
Other titles not selected for display are
- Surgical management of dorso lumbar injuries
- Anterior approach to dorsal spine
- Transclavicular approach
- Transoral surgery
- Standard posterior fixstin of C/C2 with Hartshill ring and bone grafts.
- Cuases of backpain
- Apofix interlaminar cervical fixation clamps
- Orion Anterior cervical plate stabilixation
- Exercises to kep spine and body healthy
- Cervical corpectomy and reconstruction with author�s expandable titanium cages
Title 1: Lumbar Laminectomy
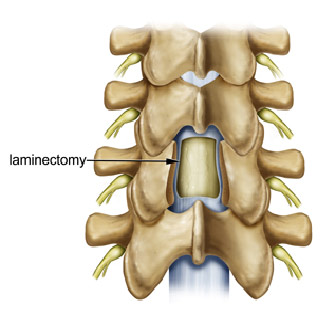
This is the basic operation on lumbar spine. It was the standard operation in the past on lumbar spine and even to day it has an important place in surgical management of several pathologies in the lumbar spine. It is a must know how for younger spinal surgeons and post graduate students.
The operative steps are clearly defined and when followed meticulously the technique will assure a safe surgical procedure much to the happiness of surgeon and the patient.
Title 2: Micro lumbar discectomy


Today micro lumbar discectomy is the gold standard treatment for a given patient of herniated lumbar disc. Surgery for herniated lumbar disc is most common all over the world.Micro lumbar discectomy is the standard procedure practiced to day. It is microscopic approach and the surgeon must know how to use the microscope and the micro instruments. It is advisable to do a micro surgery course before attempting micro lumbar discectomy.
The surgery is very satisfying to the surgeon and gratifying for the patient with early mobilization within hours of surgery and discharged home on the same day in the evening or next day in the morning. Early return to original job is one of the important aspect of this surgery.
Title 3: Internal Decompression for Spinal Stenosis (IDSS)
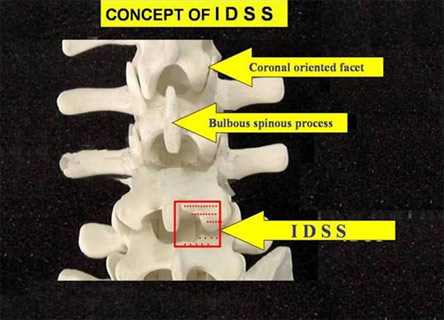
The author has popularized and developed his own technique to do internal decompression for spinal stenosis (IDSS). It is a micro technique and familiarity with microscope is most important. In a given patient with lumbar canal stenosis the spine can be effectively decompressed by this technique without compromising on its stability or integrity. Posterior segments of motion segment are preserved and cause less fibrosis in the lumbar canal. It is used effectively in younger patients but it is most effective and comforting for elderly patients with multiple level stenosis. They can be mobilised very quickly. The prognosis is good and on the whole it is a popular and useful technique.
Title 4: Posterior lumbar interbody fusion (PLIF)
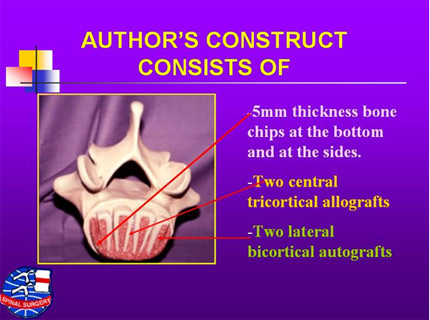
Posterior lumbar interbody fusion is popularized by the author in India. He developed his own construct for interbody fusion which became popular and the author is sometimes referred to as PLIF Ramani instead of PS Ramani.
Author at first did uninstrumented PLIF as instruments then were not available. The author had to establish a bone bank. Over the years technology improved and instrumented PLIF became popular and now is being used all over the world. Instruments commonly used are pedicle screws and rods with interbody cages. Further technological progress has seen the use of percutaneous screws and change over from PLIF to TLIF.
Instability in the lumbar spine is extremely common specially in elderly patients. PLIF is mandatory to stabilize the spine.
Title 5: Pedicle screws and rods (plates) for fusion
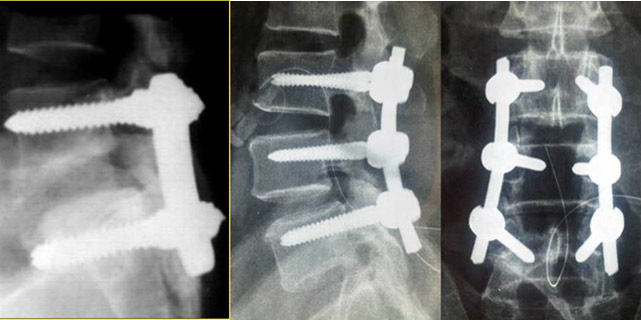
Pedicle screws are now universally used for stabilization for the spine. To begin with, after 1985, Acromed VSP plates and screws were used. Now, screws and rods are used and several companies have their minor modifications. The learning curve is simple and short. However caution is mandatory as at least 5% of the screws are misplaced. Commonest cause of misplacement is breach in the continuity of pedicular cortex medially and inferiorly causing irritation of the nerve root. The operative technique must be known by all senior resident, junior and senior doctors because of its popularity and frequency of use. The Titanium metal is MRI compatible. The technology now is changing from open to percutaneous but one must acquaint oneself with the open technique first.
Title 6: ChronOS strip

Degenerative lumbar canal stenosis with or without instability is extremely common once age advances. The main pathology originates in the facet joints and they are hypertrophied and coronally oriented causing significant lateral recess stenosis. Decompression with or without pedicle screw stabilization can give tremendous relief to the clinical symptoms of the patient but what about facet degeneration? Relentless progression of the degeneration of facet can cause overgrowth of the bone along the excised borders of the laminae resulting in canal stenosis, recurrence of symptoms and re-surgery for decompression to get reief of symptoms once again. Can we attempt to stop this degeneration? A fused joint of the spine (facet joint) is stable and does not cause osteophyte formation or hypertrophy of the bone. Following decompression Laminectomy, the author has attempted to fuse the facet joints and achieve bony fusion with the use of ChronOS strip which is nothing but ChronOS granules bound together with a sticky bio-compatible glue so the granules are transformed into a stripwhich can be fixed sub periosteally to the facet joints in a n attempt to cause fusion. Short term clinical results are good. Long term clinical results and fusion of facet joints need to be studied.
Title 7. PDS for Interspinous
stabilization of the Spine in degenerative lumbar canal stenosis causing early moderate instability

The spinal surgeons are now convinced that for moderate instability, it is not necessary to use strong pedicle screw instrumentation for stabilization. Lighter assemblies like interspinous stabilization with a device can be adequate following IDSS. Several varieties of interspinous stabilization devices are available in the market. The author has preferred to stick to one device �Synthes InSpace�. Its breadth is fixed but the diameter can vary depending of availability of space between the two spinous processes. Devices with different measurements are available. 12mm broad is the standard device and 14 being the next common. It is inserted percutaneously through a small stab incision 10 cm away from the midline. The device is dynamic. It allows normal motion of the spine and prevents abnormal mobility. It also transfers weight bearing from the intervertebral disc from anterior to posterior with the result that the intervertebral disc is not stressed. The mobility if the spine is not affected and with the use of InSpace device, if felt necessary, it can be removed any time without any implications.
8. Myelomeningocoele
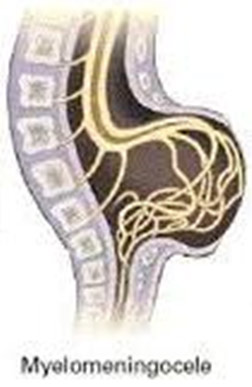
A common spinal surgery in the newborn and the infants. The risk of the surgery lies in the fact that nervous issue can be freel mixed or stuck t the sac of meningo myelocoele and the fibres of the cauda equine might have migrated into the sac of the myelocoele. It is very important to understand the concept so that the nerve roots are not damaged causing neurological deficit. Done meticulously, preferably with the use of microscope, the surgery for the meningomyelocoele can be rewarding. Since the child is young, the surgical procedure demands extreme co operation from the anesthetist.
9. Anterior cervical fusion (ACF)

Cervical Spondylosis is becoming very common even in the younger population. The pathology lies anteriorly and the herniated disc can be excised meticulously by anterior approach. The author has always believed to interpose a bone graft or a metallic cage in the space to achieve fusion. Anterior approach is simple, once the carotid sheath is retracted laterally and the hollow organs are retracted medially. Presence of blodd vessels and several nerves causes apprehension in the younger spinal surgeon but with familiarity they can realize that the approach is very simple. The author has always preferred to use horizontal skin incision and he has devised cages for interbody fusion of the cervical spine. For one level fusion it is not necessary to use cervical plate. In two level fusion it is preferable to use a plate. It has no blood loss and the surgery is very clean. Position of the neck is very important for easy access to the anterior surface of the cervical spine.
10. Use of cervical plate in interbody fusion
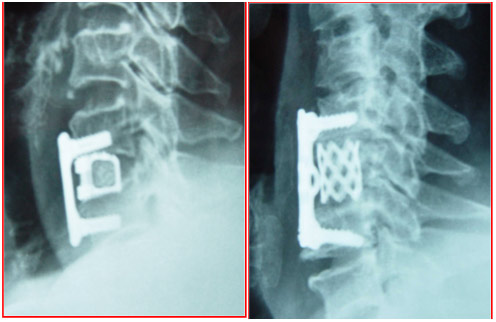
With 2 level or more cervical interbody fusion it is mandatory to use cervical plate. It provides rigid stabilization with no fear of cage being slipped out. However, it compromises the mobility of the spine and can be responsible for adjacent segment degeneration. Several varieties of plates are available with locking screws and predetermined direction of the screw. The plate must be fixed snuggly so that it is not displaced. In multilevel cervical fusion, it is mandatory to see under fluoroscopy that the lordotic curvature of the spine is maintained. The spine sould not be fixed in straight position or over extended position.
11. Posterior cervical microdiscectomy
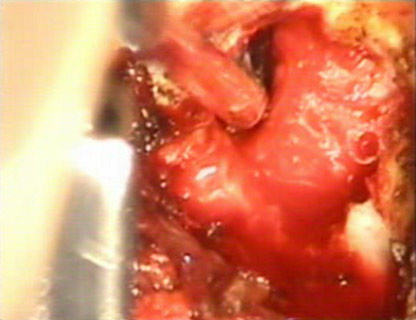
This is a microscopic procedure and similar to microlumbar discectomy described above. The author has devised special cervical retractor for this procedure. It can be done in sitting position or prone position. It is most suitable in younger patients with posterolateral herniation of the disc. The technical point to remember is that many times the disc is herniated in the axilla of the nerve root. The integrity of the spine is maintained, the procedure does not cause instability and there is no need for any type of fusion of the spine. It is a minimally invasive procedure and the patient can be sent home on the same day in the evening or next day in the morning. The spine is mobile, and there is no need for cervical collar. Cervical muscle strengthening exercises are mandatory.
 11 Posterior Cervical Microdiscectomy
11 Posterior Cervical Microdiscectomy
 10 Use of Cervical Plate in Interbody Fusion
10 Use of Cervical Plate in Interbody Fusion
 09 Anterior Cervical Fusion (ACF)
09 Anterior Cervical Fusion (ACF)
 08 Myelomeningocoele
08 Myelomeningocoele
 07 Interspinous Stabilization of the Spine
07 Interspinous Stabilization of the Spine
 06 ChronOS Strip
06 ChronOS Strip
 05 Transpedicular Screws & Rods (Plates) for fusion
05 Transpedicular Screws & Rods (Plates) for fusion
 04 Posterior Lumbar Interbody Fusion (PLIF)
04 Posterior Lumbar Interbody Fusion (PLIF)
 03 Internal Decompression for Spinal Stenosis (IDSS)
03 Internal Decompression for Spinal Stenosis (IDSS)
 02 MICRO LUMBAR DISCECTOMY
02 MICRO LUMBAR DISCECTOMY
 01 LUMBAR LAMINECTOMY
01 LUMBAR LAMINECTOMY